Emergencies in pediatric oncology Superior vena cava syndrome
Definition
Superior vena cava syndrome is a group of symptoms caused by obstruction of blood flow through the superior vena cava (SVCS). A patient with SVCS requires immediate diagnostic evaluation and therapy.
Superior mediastinum syndrome is a combination of symptoms caused by SVC compression with blood flow obstruction plus compression of the trachea. The both syndromes usually occur together.
Due to anatomy of the upper respiratory tract in children (they have significantly narrower airways in comparison with adults) is SVCS severe life threatening emergency in pediatric oncology.
Pathogenesis
The superior vena cava (SVC) is the major drainage vessel for venous blood from the head, neck, upper extremities, and upper thorax. It is located in the middle mediastinum and is surrounded by relatively rigid structures (sternum, trachea, right bronchus, aorta, pulmonary artery, and the perihilar and paratracheal lymph nodes). SVC is a thin-walled and low intraluminal pressure vascular structure.
There are three mechanisms of pathogenesis SVCS:
- thrombosis of SVC
- obstruction of SVC by intrinsic pressure and direct tumor invasion to the venous wall (frequently associated with secondary intravascular thrombosis)
- compression of SVC - extrinsic pressure of a tumor mass against the relatively thin-walled SVC.
Complete SVC obstruction is common as a result of extrinsic compression in combination with intravascular thrombosis. Incomplete SVC obstruction is more often secondary to extrinsic compression without thrombosis.
The main problem of SVCS is impaired return of venous blood from the drainage areas (head and neck, upper extremities and upper thorax) (Figure 1).
Despite collateral pathways are activated, venous pressure is almost always elevated in the upper compartment if obstruction of the SVC is present.
Clinical presentation, symptoms
Initial partial obstruction of superior vena cava (SVC) may be asymptomatic, but more often, minor symptoms and signs are overlooked. With further progression of SVC obstruction the symptoms and signs become more obvious (Figure 2).
- Respiratory symptoms: initially started as orthopnea, later on progressed to dyspnea. Dyspnea together with dry nonproductive cough is the most common symptom observed in almost 75 % of patients with SVCS. Sometimes is also hoarseness and dysphonia or stridor, shortness of the breath and chest pain.
- CNS symptoms: present as so called „wet brain syndrome“ with headache, visual changes – blurred vision, cognitive disturbances, syncope, stupor, seizures, impaired consciousness
- Venous obstruction is present as facial swelling, plethora or cyanosis of the face, head fullness, arm swelling, full jugular veins, engorgement of collateral veins , suffusions of the conjunctiva (Figure 3).
All symptoms of SVCS in children progressed rapidly in hours and days, median 3 to 7 days.
Diagnostic procedures
Diagnosis of SVCS is usually based on clinical and physical examination of the patient and history of symptoms.
Physical examination: show the characteristic physical findings of SVCS mentioned above. Bending forward or lying down may aggravate the symptoms and signs. Usually is no palpable pulsation on carotid veins.
The simple clinical test for SVCS: brachial veins remain full if right arm is raised above patient’s head.
Laboratory tests: may be helpful in diagnosis and differential diagnosis of underlying cause of SVCS.
- complete hematology tests: CBC including microscopic differential count , coagulation profile and flow-cytometry of peripheral blood
- biochemistry: renal and liver function tests, uric acid, LDH, minerals due to risk of acute tumor lysis syndrome, acibasic balance
- tumor markers: are important for differential diagnosis of tumor (AFP,β-HCG, NSE, catecholamines in urine )
- bone marrow biopsy: is an important part of initial work up for differential diagnosis of mediastinal mass
Imaging studies:
Patients presenting with superior vena cava syndrome (SVCS) may be diagnosed by means of physical examination alone. However, subtle presentations necessitate diagnostic imaging.
Chest X-ray: both projections (anteroposterior and lateral) may reveal a widened mediastinum or a pathology mass localised in the mediastinum. Mediastinal mass on X-ray is always indication for CT scan (Figure 4).
Computer tomography (CT) has an advantage of providing more accurate information regarding location and size of the pathology mass, its character, vascularisation, calcifications etc. It also provides information on other critical structures, such as the bronchial tree, trachea, pericardial or pleural effusion.
MRI: is not routine or standard method in initial work up for mediastinal pediatric tumors,
Histopathology:
Histopathology is the key for diagnosis, treatment and prognosis of patient with SVCS. The basic rule is to use the least invasive method of diagnosis. The aim is to avoid general anesthesia due to risk of respiratory insufficiency requiring mechanical ventilation.
Therefore in case of peripheral lymphadenopathy is preferred extirpation of peripheral lymph node in local anesthesia together with bone marrow biopsy.
Differential diagnosis of mediastinal tumors
The clinical presentation of SVCS is clear, but it is necessary to differentiate primarily causing disease. Slowly growing tumors even with large mediastinal mass may not lead to the acute development of SVCS. The history of disease, the first symptoms and duration of the problems are very important for differential diagnosis.
Differential diagnosis of most frequent causes of SVCS in pediatric oncology is shown in Figure 5.
Benign mediastinal tumors in childhood (neurofibroma, desmoid, mature teratoma, hamartoma) usually grow slowly and therefore do not cause SVCS.
Nonmalignant conditions that can cause SVCS are extremely rare in pediatric population.
Therapy
In the management of superior vena cava syndrome (SVCS), the goals are to relieve symptoms and to attempt cure of the primary malignant process. In pediatric oncology (unlike adult oncology) a high percentage of patients with rapid-onset obstruction of the superior vena cava (SVC) are at risk for life-threatening complications. Therapeutic approach is determined by the severity of symptoms and type of primary mediastinal tumor.
General guidelines for pediatric patients with SVCS plus supportive care:
- patient with clinical evidence of SVCS must by immediately send to specialized center of pediatric oncology and admitted to ICU with vital signs monitoring, fluid balance monitoring every 4 – 6 hours
- hydration (CAVE overhydration worsening the symptoms of SVCS) via central venous catheter inserted to femoral vein (AVOID catheter insertion to SVC basin)
- conservative treatment measures (elevation of the head and neck at the angle minimum 45 degrees), supplemental oxygen and diuretics
Causal treatment of primary tumor: has to be started as soon as the confirmation of histological diagnosis
- corticosteroids: in gradually increasing doses have a rapid effect, but never is recommended prior to collection of tissues for histological examination. Even one dose of corticosteroids may substantially influence further progression and prognosis of the patient with lymphoma/leukemia by induction of corticoresistance.
- chemotherapy: chemotherapy for pediatric malignant mediastinal tumors leading to SVCS is the key treatment modality. In the case of life-threatening SVC obstruction chemotherapy can begin immediately (after the collection of material for histology) from vital indication (so called not fall submission). Effect of chemotherapy is viewable in the timeframe hours to days.
- radiotherapy: radiotherapy in children with SVCS is practically not indicated and not used in pediatric oncology. Radiotherapy is indicated only in case of serious airways obstruction and threatening brain edema. In adult oncology it is used as the initial treatment if a histologic diagnosis cannot be established and the clinical status of the patient is deteriorating.
- thrombolytic treatment: patients with thrombosis of SVC may be treated with thrombolytic (eg, streptokinase, urokinase, or recombinant tissue-type plasminogen activator) or anticoagulants (eg, heparin or oral anticoagulants)
Surgical treatment: for hematology malignancies (leukemia/lymphoma) surgery has only diagnostic role (biopsy). Some surgical method could be used in palliative intention for SVCS when radical resection of the tumor is not possible or tumor not responding to chemo/radiotherapy.
- bypass: is surgical method for highly selected group of the patients with chronic symptoms of SVCS caused by non – malignant diseases (tuberculosis, sarcoidosis) or inoperable benign tumors not responding to treatment (aggressive fibromatosis, neurofibromas)
- surgical stent: leads to rapid clinical improvement within few days in patients with inoperable tumor not responding to anti-neoplastic therapy. In pediatric oncology this method of SVCS treatment is not used.
Prognosis, outcome
SVCS is among acute life-threatening conditions in pediatric oncology. The most common cause is hematologic malignancy. Prognosis SVCS depends on the underlying disease (survival correlate with histology) and response to treatment. For chemosensitive tumors in children (non-Hodgkin lymphomas, leukaemia, germ cell tumors) the prognosis is usually excellent, SVCS symptoms disappear with the response of the tumor to the causal treatment over few days.
Author: Viera Bajčiová, MD, PhD
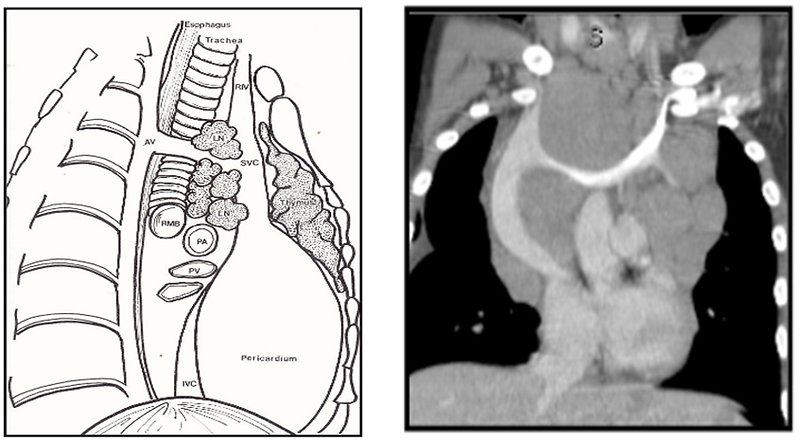 Figure 1: Patophysiology of SVCS |
 Figure 2: Clinical presentation and symptoms of SVCS |
 Figure 3: Clinical presentation of SVCS – edema of the head and neck |
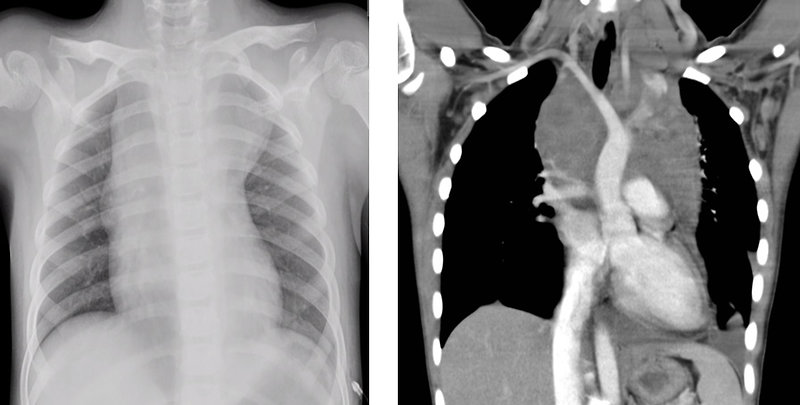 Figure 4: Chest X-ray and CT scan of mediastinal NHL |
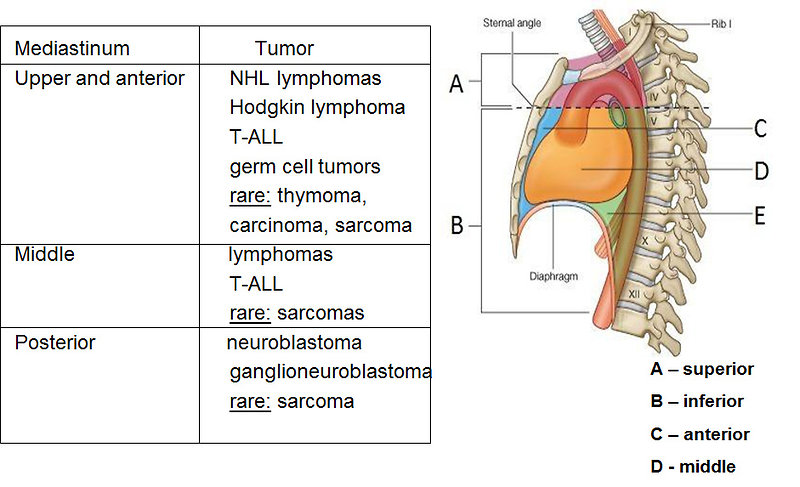 Figure 5: Differential diagnosis of mediastinal tumors in pediatric oncology |
|||