General section
Author:
Viera Bajčiová, MD, PhD
1.1 History of pediatric oncology
Cancer is not a new disease of the modern era, but it is as old as humanity itself. The world’s oldest documented case of cancer hails from ancient Egypt in 3000 b.c. (8 cases of breast tumors were recorded on the papyrus).
Pediatric oncology is a relatively new medical discipline. It started to become independent from the adulthood oncology in the sixties of the 20th century. Existence of pediatric oncology is based on an understanding of the fundamental differences between the tumors of children and adults.
For historically short existence of pediatric oncology dramatic and significant progress has been achieved in treating pediatric cancer patients. Currently it is possible to successfully cure over 85% of children and adolescents with cancer (Figure 1).
Importance of pediatric oncology determines:
- mainly the object of interest – malignant disease of the youngest part of the population.
- although cancer in children is rare, in economically developed countries pediatric cancer is the 2nd leading cause of death among children under 15 years of age after accidents. Pediatric cancer is therefore the most common disease leading to death in children despite the fact that most of the pediatric tumors are curable in a high percentage (Figure 2).
1.2 Epidemiology of childhood cancer
Childhood cancer make up less than 1% of all cancers in the population diagnosed each year.
Incidence: the world age-standardized incidence rates were typically in the range 70-160 cases per million children per year, but incidence and mortality rates of childhood cancers differ worldwide.
Geographic differences depend on how extensively data are reported.
- United States: the overall incidence of childhood cancer is about 125 per million
- United Kingdom: incidence is about 130 per million
- Europe: the incidence rates were highest in Northern Europe (Finland, Denmark) and Italy, about 170–180 per million (Figure 3)
Gender and race: the highest incidence is in white males followed by Hispanic males. The boys are affected by cancer more frequently than girls in all races (Figure 4).
Age: the highest incidence rates for all children's cancers combined are in the under-five for both sexes, with almost half (47%) of all children's cases being diagnosed in this age group. This pattern varies greatly by cancer type (Figure 5).
Mortality rate of childhood cancer is decreasing together with significant dramatic improvement of overall survival (Figure 6). Mortality rate depends most of all on tumor type and extent of disease (Figure 7).
1.3 Etiology of childhood cancer
Cancer is assumed to be multivariate, multifactorial disease that occur when a complex and prolonged process involving genetic and environmental factors interact in a multiple sequence.
Pediatric tumors differ in many ways from the tumors in adulthood, and therefore underlying causes may be different. But the molecular mechanisms of carcinogenesis are the same in any age. The tumor is essentially a genetic disease, some 500 genes plays a role in the development of a tumor (Figure 8).
Sporadic occurrence (80–90 %) of pediatric tumors without known cause of cancer.
Hereditary dependent tumors:
- adults 5-10%
- children prerequisite to 18-20%
Around 75 hereditary cancer predisposition syndromes associated with pediatric cancer have been described, most of them are rare with autosomal dominant transmission. Knowledge of hereditary syndrome is important not only for the child but also for the family members (Figure 9).
Familial occurrence (a gene-environment interactions, low penetrating genes, the role of specific genes, but inherited predisposition is not precisely defined ) could be associated with some type of the tumors (familial melanoma)
Congenital malformations and inborn errors are frequently associated with different types of the cancer depend on type of congenital malformations
Immunodeficit:
- primary (inherited) – Wiscott-Aldrich syndrome, ataxia teleangiectatica
- secondary after immunosuppressive therapy (organ transplant)
Environmental factors in pediatric oncology have only a minor role. The effect of external environmental factors is affected by the duration of exposure and does not explain the existence/development of tumors in infants and children under 5 years of the age. Their impact on children's cancer development is indirect - parental exposure and possible mutations in parents (Figure 10).
- ionizing radiation (secondary bone tumors, thyroid cancer …)
- chemicals (asbestos, pesticides, cockayne, heavy metals…)
- ultraviolet light (malignant melanoma and skin carcinomas)
-
infectious agents specially viruses:
- hepatitis B/C virus – associated with hepatocellular carcinoma
- EBV – associated with endemic Burkitt lymphoma, Hodgkin lymphoma, nasopharyngeal carcinoma
- HPV type 16 – associated with carcinoma of the cervix, vulva, vagina, anus, papillomatosis, carcinoma of oro and nasopharynx
- HTLV-1 – associated with AIDS, Kaposi sarcoma, lymphoma
- life style factors (tobacco smoking, diet, stress, obesity….)
1.4 Differences between pediatric and adult oncology
Pediatric oncology differs from oncology of adulthood in two main areas:
- malignant tumor itself
- child as an oncology patient
Tumor itself:
-
age specific histologic types of pediatric tumors differs from the others age groups.
- Embryonal types of the cancer are tumors characteristic for the early life (0 – 5 years). The initiation of the tumor (= the first genetic hit) occured usually prenataly during embryonal life. Embryonal tumors origin from undifferentiated tissues and retain the embryonic rapid growth (hepatoblastoma, retinoblastoma, neuroblastoma, nephroblastoma etc.).
- Mesenchymal tumors (sarcomas) are typical for adolescent age, origin from soft tissues or bones.
- Epithelial tumors (carcinomas) are extremely rare in pediatric age, represent only 2% of all malignancies in children up to 15 years of the age and 12% in adolescents (thyroid carcinoma, adrenocortical carcinoma)
- The most frequent malignancies in children up to 15 years of the age are on (Figure 11)
-
biological behavior of pediatric tumors:
- pediatric tumors are highly malignant with rapid growth (doubling time within hours and days rather than weeks or months) and rapid locoregional involvement
- early metastatic (hematogenous or lymphogenous) spread
- growth fraction of the tumor and proliferation index is very high
- therefore pediatric tumor is considered an acute life-threatening condition
- symptoms in children are usually nonspecific
- due to biological aggressiveness of pediatric cancers they are generally very well chemosensitive and radiosensitive with a good therapeutic response
- premalignant stage ( tumor in situ) is not recognizable in pediatric tumors (Figure 12)
- ICCC classification. Tumors typical for adult age are classified according to the location of the primary tumor (colon cancer, lung cancer etc.) based on the International Classification of Diseases, ICD - O classification (International Classification of Diseases for Oncology). Childhood cancers are further classified into cancer type using the International Classification of Childhood Cancer (ICCC), which takes the tumour's anatomical site and morphology into account. The ICCC divides childhood cancers in 12 cancer types (called diagnostic groups), currently in force 3rd edition (Figure 13).
Child:
Child's organism is not a “miniature adult”. Child is not only growing, but still evolving individual. On the one hand maturing organs and tissues (eg. brain) in many ways limits the choice of treatment options and anticancer treatment has a potential risk of late effects and complications. Factors influencing risk of late effects:
- age of the child at the time of anticancer therapy
- mutilating surgery ( amputation)
-
type of therapy
- radiotherapy (cumulative dose of irradiation, localisation and irradiation field)
- chemotherapy (type of chemotherapy, cumulative dose)
- combination radio and chemotherapy
On the other hand, children do not have comorbidities and compared to the adults they tolerate intensive chemotherapy significantly better, regenerative processes are much faster.
1.5 Clinical presentation of childhood cancer
Clinical presentation of childhood cancer depends on:
- age of the patient
- type of tumor, size and growth pattern
- localization of tumor (origin)
- metastases and their localization
None of the symptoms are specific for malignancy and may be caused by a variety of other causes. Any symptom not responding to adequate treatment and lasting longer than 2-3 weeks, for which is no other explanation, should raise suspicion of a malignant tumor (Figure 14).
- local symptoms: palpable mass, compression of surrounding organs and tissues, local pain, redness, intracranial hypertension, intestinal/urinary obstruction, caugh, stridor…
- systemic symptoms: failure to thrive, weight loss, fever, changes in locomotor stereotype, sweating, weakness, fatigue….
-
paraneoplastic symptoms: are not so frequent and differs comparing with adult tumors:
- watery diarrhea (VIP production) in neuroblastoma
- carcinoid syndrome (serotonin production) in carcinoid
- gynecomastia in testicular cancer
- thrombocytosis in hepatoblastoma (thrombopoietin production)
- virilism or pseudopubertas praecox (adrenal or gonadal stromal tumors)
1.6 Treatment modalities
The decreased mortality rate of pediatric cancers has been one of the major success stories of medicine in the last 30 years. Improvements in the survival rates of leukemias, Hodgkin disease, and sarcomas have been notable successes. Most of these improvements can be traced to the use of aggressive multimodal therapy and improved supportive care to prevent and treat infections.
1.6.1 Surgery
Surgery is very important and for some tumors also curative treatment. The most important fact is, that surgery is a local treatment leads to local control for the most of the tumors. If radical tumor resection is not possible, usually it means a higher risk of local recurrence or relapse. There are very precise well defined surgical guidelines for most of the tumors. Principles of surgical therapy in pediatric oncology:
- correct surgical access (nephrectomy due to Wilms tumor is recommended via laparotomy , not via lumbotomic access)
- peroperative staging ( visual control, palpation and sampling of regional lymph nodes or any suspicious lesion)
-
type of surgery:
- R0 – radical resection, resection margins are free of tumor (Figure 15)
- R1 – marginal resection (microscopic residual tumor)
- R2 – macroscopic residual tumor
- partial resection/debulking – reduction of tumor mass
- biopsy
- timing of radical surgery:
- primary (initial) surgery
- delayed surgery (after neoadjuvant chemotherapy)
1.6.2 Chemotherapy is the most effective systemic therapy of pediatric cancer, to treat cancer throughout the body. Chemotherapy is cell cycle specific medication and kills actively dividing cells. Unlike healthy cells, cancer cells grow continuously because they don't respond to normal signals that control cell growth. Chemotherapy works by disrupting cell division and killing actively dividing cancer cells (Figure 16). In pediatric oncology treatment protocols almost always use combination therapy, which is the use of two or more cancer-fighting drugs. This combination of cytotoxic therapy lessens the chance that the cancer will become resistant to one type of drug and improves the chances that the cancer will be cured.
1.6.3 Radiotherapy is another effective local therapy of cancer and treats the cancer in irradiated area. Radiotherapy should be used in curative or palliative indication. In pediatric oncology indications for radiotherapy have been significantly reduced over the years due the significant risk of late complications.
Limiting factors for radiotherapy :
- tumor radiosensitivity
- radioresistance of surrounding organs
- size of radiation field and cumulative dose of RT
- age of child
- combination with chemotherapy (some agents may be used as radiosensitisers)
Modalities of radiotherapy:
- stereotactic radiotherapy
- peroperative radiotherapy
- conformal radiotherapy
- linear accelerator
- proton radiotherapy
- hyperfractionation
- brachytherapy
1.6.4 Biology targeted therapy: The main goals of medical research and development of the new treatment modalities in pediatric oncology are:
- improvement of overall survival
- reduction of disease/treatment related morbidity and mortality
- reduction of the late effects of anticancer therapy
Modern biology targeted anticancer therapy in pediatric oncology has 3 – 5 years delay comparing with the adult age oncology for several reasons:
- Rarity of pediatric cancer in the population
- Effective standard oncology treatment (chemotherapy) (Figure 17)
- Recurrent or resistant pediatric tumors are so called ultra-orphan diseases
- Limited information and biology studies of pediatric tumors
- Lack of age specific pediatric clinical trials
Scientists ideally would like to find methods of treatment that are more specific to killing just the cancer cells and not affecting surrounding healthy tissues. With new informations about the mechanisms of cell replications, carcinogenesis, cellular metabolic pathways oncologists are able to stop the growth of, or even kill specifically the cancer cells. Because these biological molecules important for cancer cell processes and metabolism are called “molecular targets,” this therapy is sometimes called “molecular targeted therapy”. By altering molecular and cellular changes that are specific to cancer, targeted cancer therapies may be more effective than current treatments and less harmful to normal cells (Figure 18).
1.6.5 Immunotherapy is treatment that uses certain parts of a person’s immune system to fight diseases such as cancer (Figure 19). This can be done in several ways:
- stimulating patient own immune system to work harder or smarter to attack cancer cells (active immunotherapy)
- giving patients’ immune system components, such as man-made immune system proteins (passive immunotherapy)
In the last few decades immunotherapy has become an important part of treating some types of cancer (malignant melanoma, lung cancer, renal carcinoma).
The main types of immunotherapy now being used to treat cancer include:
- monoclonal antibodies (rituximab, bevacizumab,denosumab, vemurafenib….)
- immune checkpoint inhibitors (anti CTLA-4 and anti PD-1): these drugs basicallytake the ‘brakes’ off the immune system, which helps it recognize and attack cancer cells (anti CTLA-4 ipilimumab, anti PD-1 nivolumab) (Figure 20)
-
adoptive cell immunotherapy:
- allogenic bone marrow transplantation, graft versus leukemia effect
- cancer vaccines (dendritic cells )
-
activation of innate immunity:
- cytokines and growth factors (interferon α, interleukin-2, tumor necrosis factor α)
1.6.6 Supportive therapy is very important part of anticancer treatment in pediatric oncology due to aggressiveness of treatment protocols. Supportive treatmens means therapy of complications caused by tumor itself or anticancer therapy. Supportive treatment includes:
- Therapy of infectious complications ( febrile neutropenia, sepsis, septic shock
- Therapy of bleeding and coagulation problems ( disseminated intravascular coagulation)
- Antiemetic therapy
- Analgetic treatment
- Nutrition support
- Treatment of polyneuropathy
- Psychological and psychiatric support
- Physical exercises
1.7 Organization of pediatric oncology care
Due to the biology of pediatric tumors generally applies rule in pediatric oncology is to treat each patient with curative aim. Palliative approach is rather rare.
Significant progress has been made in the treatment results of pediatric cancer and this progress is possible because of national centralized care and close international cooperation.
1.7.1 Pediatric cancer centers provide the specialized care coordinated by a team of experts experienced on pediatric cancer. Multidisciplinary expert team know the unique need of pediatric cancer patients and their families (Figure 21). These centers offer the most up-to-date treatment of all types of pediatric cancer. Based on recommendation for centralized oncology care is the ideal situation of one pediatric oncology center to 5–7 million inhabitants.
1.7.2 Clinical trials represent one of the methods how to achieve progress in treatment of pediatric cancer and one of the mode to get state-of-the-art treatment for children and adolescents with cancer. For some types of the cancer it is the only way to get access to some new modern types of treatment. Multicentric clinical trials due to rarity of pediatric cancer are based on multinational and international level.
1.7.3. European standards of care for children with cancer prepared and published in 2009 by SIOP-E (International Society of Pediatric Oncology - Europe) defined the guidelines which represent the minimum standards of care that should be implemented at the EU level. Guidelines describe the different aspects of pediatric oncology care and are used as a tools for both professional and parents/patients groups. The standards are available in 16 languages
1.8 New challenges in pediatric oncology
Significant and dramatic improvement of pediatric cancer survival within last decades leads to definition of new challenges and priorities in the field of pediatric oncology.
1.8.1 Risk adapted individualized strategy: the main aim of this strategy is the exact definition of the individual risk factors for each particular child based on clinical factors (type of the tumor, clinical stage, tumor markers levels etc.) and results of biology tumor studies (cytogenetics, molecular genetics, mutation analysis, whole genome sequencing) . The goal is to reduce late side effects and complications of anticancer therapy without compromising treatment results.
1.8.2 Quality of life of childhood cancer survivors: currently more than 85% of pediatric cancer patients survive their disease. Number of pediatric cancer survivors in the population is continuously growing. One of 600 young people up to 35 years is pediatric cancer survivor and about 75% of them are experienced with one or more late effects of cancer treatment. Demographic studies showed that 35% of survivors are younger than 20 years, 46% is younger than 40 years and less than 18% is older than 40 years. The quality of life of childhood cancer survivors is the important issue and challenge for pediatric oncologists.
1.8.3 Care about adolescent cancer patients: The beginning of the new millenium brought along changes in the view on the issue of cancer in adolescents and young adults. Oncological community realized that this part of the population is "in no man land" and is somewhere between childhood and adult oncology, and does not meet the criteria for inclusion in either one of them.
Malignant tumors in adolescents represent a serious medical, psychological, ethical and economic problems. A group of patients aged adolescence has long been on the brink of interest Pediatric Oncology and almost completely out of interest in adulthood oncology. Treatment strategies often differ significantly according to the type of work - pediatric oncology using completely different methods of treatment compared to adult oncology. Range of histological tumor types, their biological properties and clinical behavior are age-specific and different from tumors of other age groups.
Tumor biology in adolescents is different compared with other age groups. In addition to tumor biology the age-specific biology of the host may play a role. The role of physiological factors and changes within puberty (hormonal changes, growth spurt, the volume distribution of adipose tissue), pharmacokinetics, and pharmacogenetics may differ from other age groups.
Treatment strategy that would be targeted to this specific age group with accepting specific
biological characteristics of the tumor and host in the future could significantly improve outcomes and prognosis of adolescents and young adults with malignant tumors.
1.8.4 The role of family in the treatment decision: diagnosis of malignancy in a child is a huge hit in the lives of the whole family. Diagnosis of cancer hitting all family members not only emotionally, but very frequently also economic situation of the family is influenced. Due to the nature of anticancer therapy, the potential risks of developing late effects and complications parents have to be involved in treatment decisions. Almost all clinical studies require a signed informed consent from parents applied not only treatment, but also invasive diagnostic procedures (biopsy, bone marrow aspiration, etc.). Parents need to feel that the medical staff considers them as partners in a team taking care for their child. Therefore discussion, communication and information is crucial for the mutual trust.
1.9 Prevention of childhood cancer
1.9.1 Primary prevention is focused on healthy population. The main goal is to reduce risk factors, prevent cancer and decrease incidence of malignant diseases. The main form of primary prevention is health education and information about healthy life style (food, smoking, obesity, alcohol etc.). The primary prevention of childhood cancer is practically impossible, because environmental factors do not play a significant role in the etiopathogenesis of pediatric tumors. For primary prevention can be considered a healthy lifestyle of parents. Primary prevention is in the hands of every man.
1.9.2 Secondary prevention is focused on early diagnosis of cancer and the main goal is to decrease advanced stage of disease and reduction of cancer related mortality. The forms of secondary prevention are preventive medical examinations, self-examination of the breasts or testicles and screening programs for risk group of population (colorectal cancer, breast cancer). For pediatric tumors screening is not a part of secondary prevention (we cannot define a risk group). For cancer in children preventive medical examination on regular basis is important part of secondary prevention. Secondary prevention performs general practitioner/family physician.
1.9.3 Tertiary prevention is prevention of secondary malignancy development in childhood cancer survivors and it is performed by oncologist.
Author: Viera Bajciova, MD, PhD
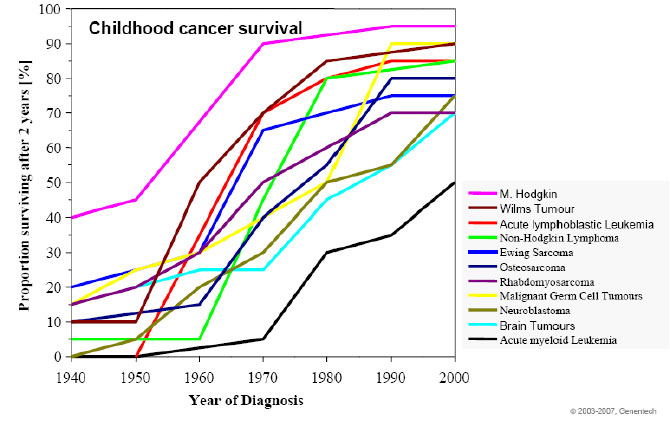 Figure 1: Improvement in childhood cancer survival |
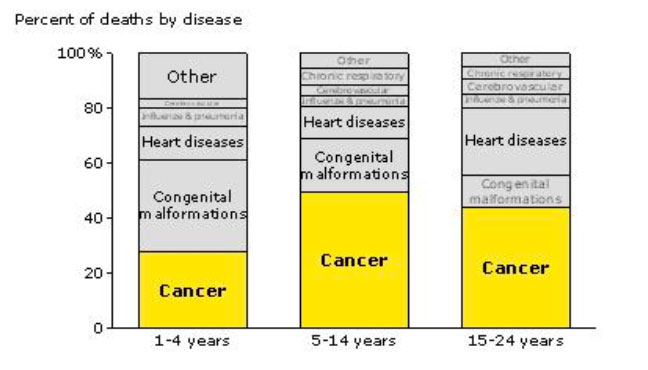 Figure 2: Cancer is the 1st cause of disease related death for children (National Academy of Sciences, USA) |
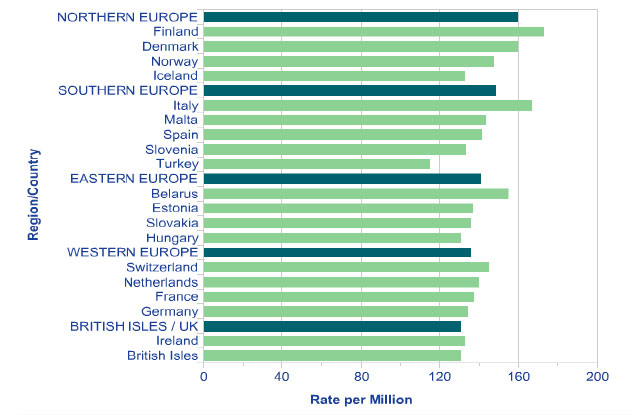 Figure 3: Cumulative risk of childhood cancer in Europe (www.who.int) |
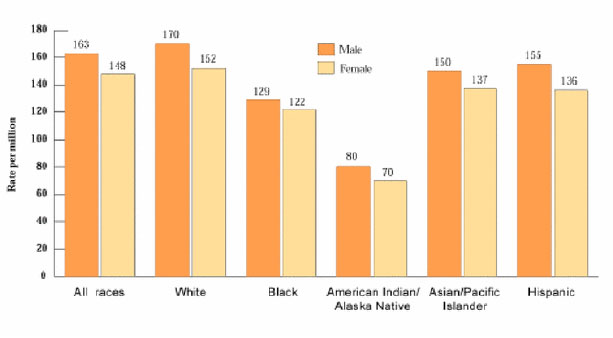 Figure 4: Incidence rates of childhood cancer by race and gender (ACS Cancer Facts and Figures, 2000) |
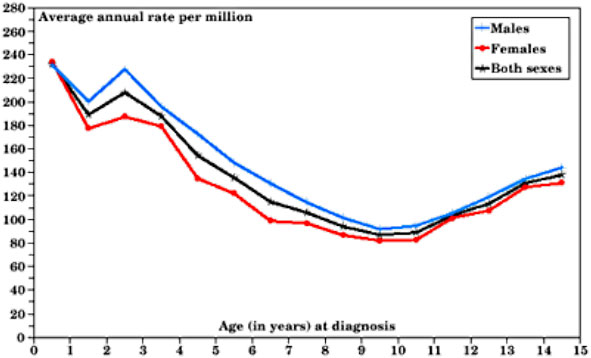 Figure 5: Total childhood age specific incidence (SEER) |
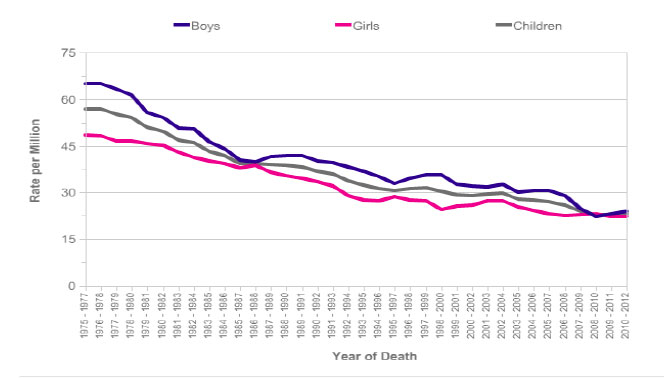 Figure 6: Mortality trends of childhood cancer over time in UK |
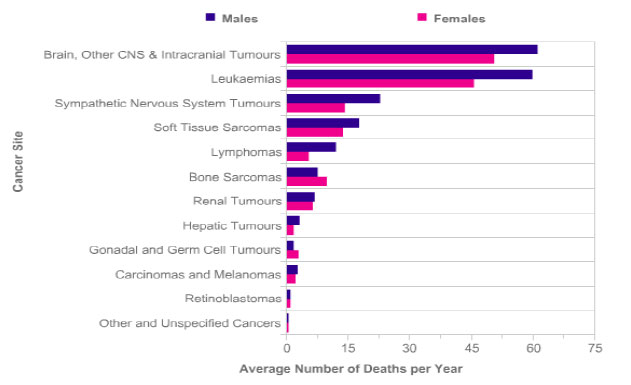 Figure 7: Mortality by tumor type in UK 1996–2005 |
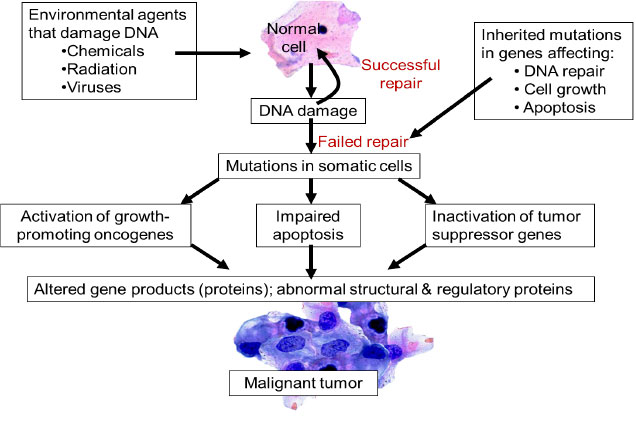 Figure 8: Overview of tumorigenesis |
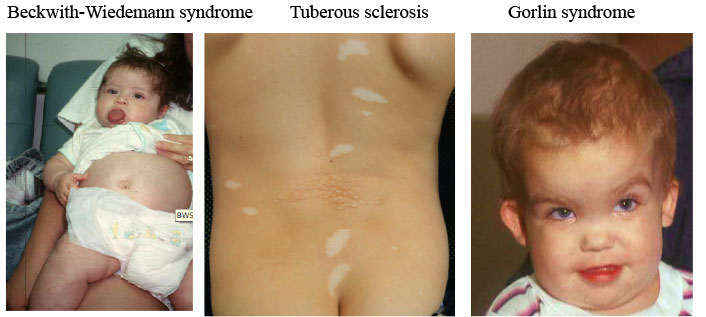 Figure 9: Genetic cancer predisposition syndromes in childhood |
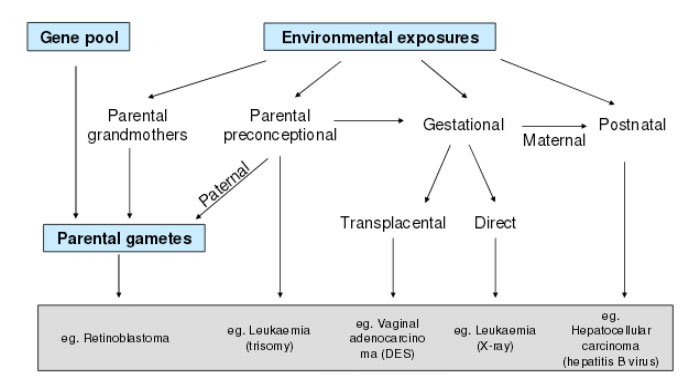 Figure 10: Possible mechanism of environmental factors to pediatric tumorigenesis (Anderson LM, Environ Health Perspect 2000) |
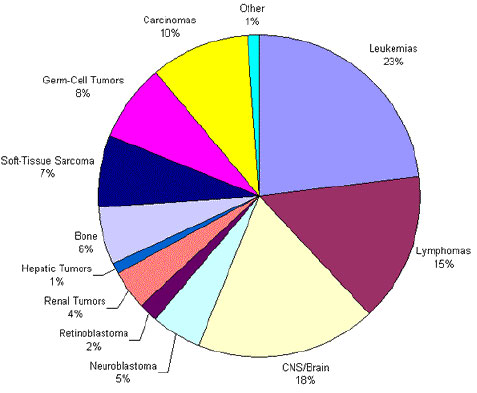 Figure 11: The most frequent pediatric tumors |
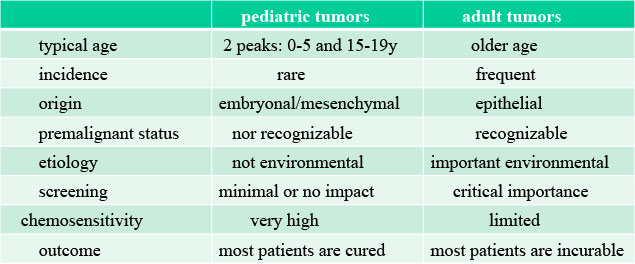 Figure 12: Cancer in children vs adults differences |
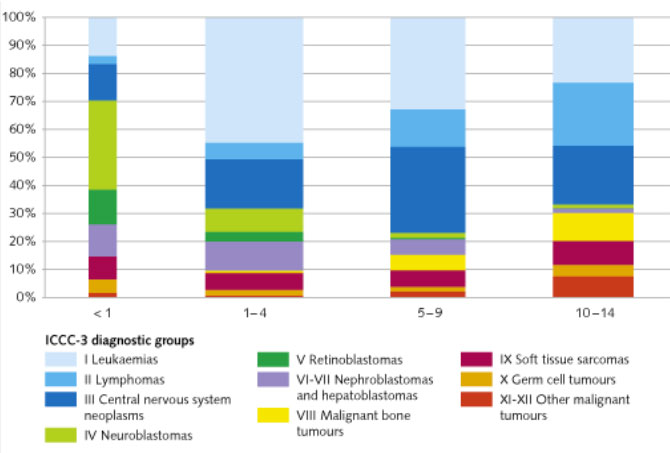 Figure 13: Pediatric cancer according to age group and ICCC classification |
 Figure 14: The most frequent symptoms of childhood cancer |
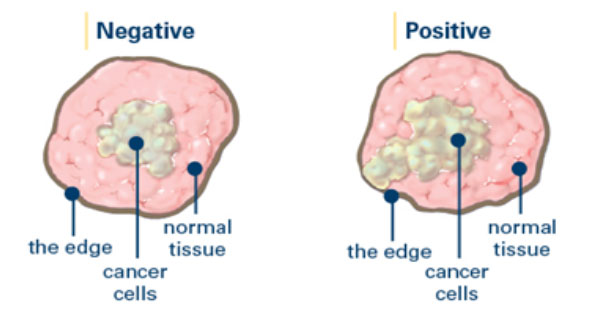 Figure 15: Surgical margins |
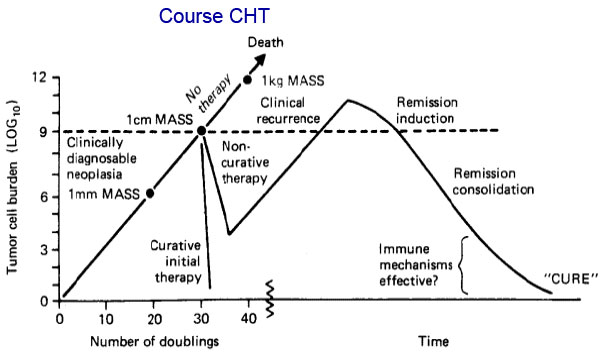 Figure 16: Effect of chemotherapy to tumor burden |
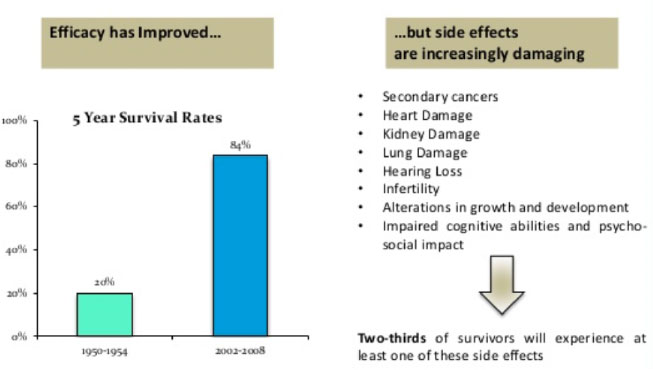 Figure 17: Improvement of treatment efficacy, but with high risk of late side effects (SEER, Cancer Statistics Review 1975–2010) |
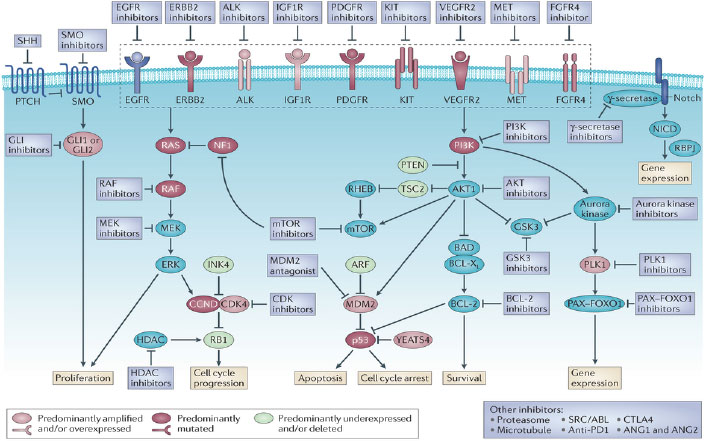 Figure 18: Targeted therapy for rhabdomyosarcoma (Kashi VP, Nat Rev Cance 2015) |
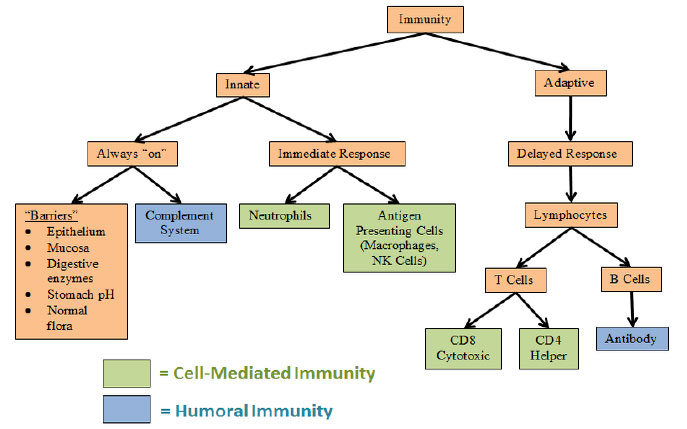 Figure 19: Structure of immune system |
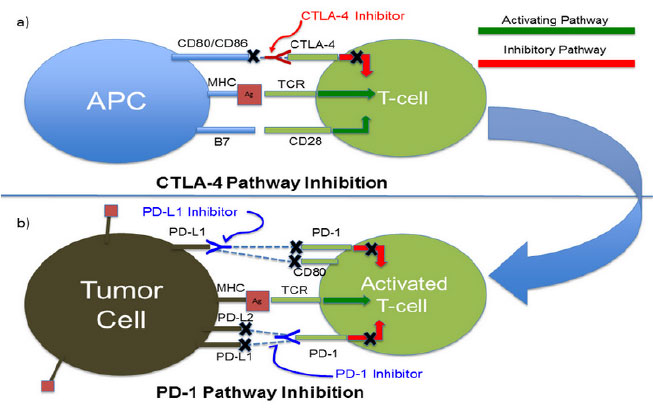 Figure 20: Immune checkpoints inhibitors (Godwin J, Discov Med, Dec 2014) |
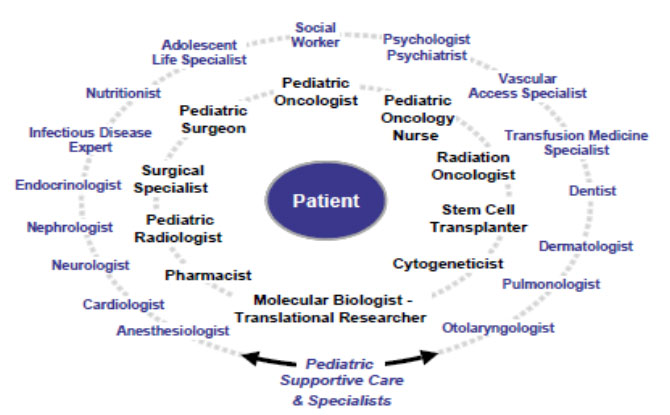 Figure 21: Multidisciplinary diagnostic and treatment team |
|||